P
Loading blog...
Loading blog...
Knowledge, Attitudes, and Practices surveys are foundational to health, social, and development research. Getting the design right requires understanding what each component is actually measuring.
Maya Chen
May 10, 2026•4 min read
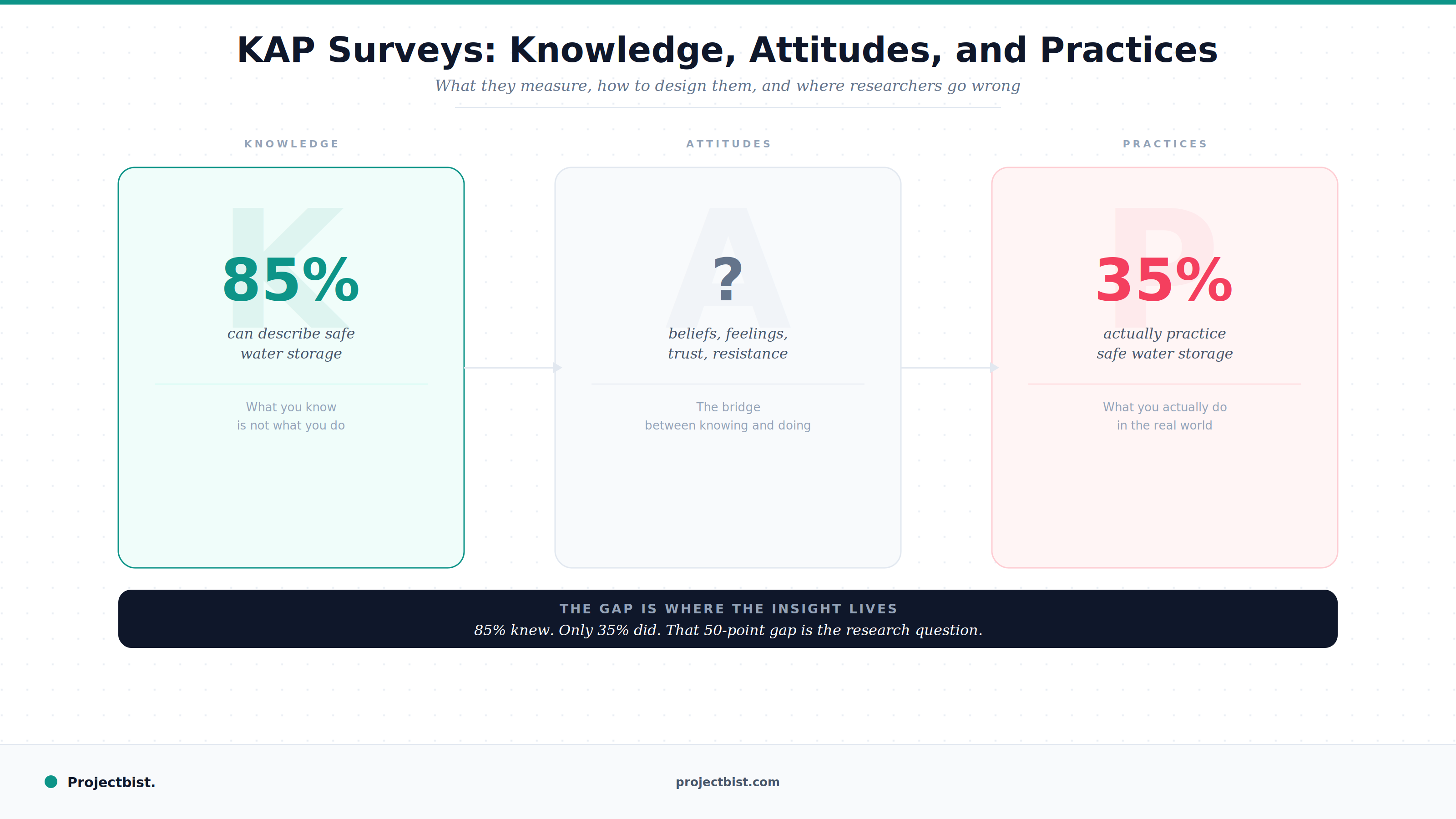
A health education program trains community members on safe water storage. After 12 months, a survey finds that 85 percent of respondents can correctly describe the proper method for storing water safely. The program is declared a success.
A follow-up assessment observes actual household water storage practices. It finds that 35 percent of the same households are actually using safe storage methods.
The gap between what people know and what people do is one of the oldest and most practically important findings in health and social research. KAP surveys, Knowledge, Attitudes, and Practices surveys, are the standard method for measuring all three components and analyzing the relationships between them.
What the respondent knows or understands about a topic. Knowledge questions have objectively correct or incorrect answers. A respondent either knows that malaria is transmitted by mosquitoes or they do not. Knowledge is measured by accuracy of recall, not by self-reported confidence.
The most common mistake in the knowledge component: asking respondents whether they know something rather than testing whether they know it. 'Do you know what causes malaria?' is not a knowledge question. 'What causes malaria?' followed by coding of the response against a correct answer list is a knowledge question.
What the respondent believes or feels about a topic. Attitudes are not true or false. They are measured on scales that capture direction (positive or negative) and often intensity. A respondent might know that vaccines protect against disease but hold a negative attitude toward vaccination based on beliefs about side effects or distrust of health institutions.
Attitude questions typically use Likert scales, agree-disagree formats, or semantic differential scales. The key design principle is that attitude items must measure one thing at a time. A compound attitude statement, like vaccines are safe and important for public health, conflates safety and public health importance in a way that makes responses uninterpretable.
What the respondent actually does. Practices are behavioral and ideally should be verified through observation rather than self-report. In large-scale surveys where observation is not feasible, practices are measured through recall: in the last seven days, did you wash your hands with soap before preparing food? The recall period should be as short as feasible for the behavior in question, since longer recall periods introduce memory distortion.
The KAP framework's value is not in measuring each component in isolation. It is in the gaps: between knowledge and attitude, between attitude and practice. Those gaps are where the intervention design insight lives.
Before writing any questions, map out what the study is trying to understand: what behaviors does the program aim to change, what knowledge deficits explain current practices, what attitudinal barriers block behavior change even when knowledge is present? This conceptual model determines what questions to include and in what order.
Knowledge questions should come before attitude and practice questions in the survey instrument. Asking a respondent about their attitudes or behaviors before testing their knowledge can prime them to answer knowledge questions more accurately than they otherwise would, inflating knowledge scores.
For well-studied health topics such as HIV, family planning, vaccination, or water and sanitation, validated KAP measurement instruments exist in the research literature. These have been tested for reliability and cultural appropriateness across multiple settings. Using them where available improves comparability and saves design time. Adapting them for local language and context is appropriate. Redesigning them from scratch is often unnecessary.
The most informative KAP analyses are not frequency distributions of each component independently. They are the cross-tabulations that reveal the relationship structure: what proportion of respondents who have correct knowledge are also practicing the behavior? Among those with correct knowledge but not practicing, what attitudinal barriers are most prevalent? These cross-tabulations directly inform program design.
What is the difference between a KAP survey and a baseline survey?
A baseline survey is a broad pre-intervention data collection tool that measures outcomes across multiple domains. A KAP survey is a specific methodology for measuring Knowledge, Attitudes, and Practices on a particular topic. Many baseline surveys include KAP components, but not all baseline surveys are KAP surveys and not all KAP surveys are baselines.
How many questions should a KAP survey include?
This depends on the topic breadth and the survey context. Most KAP surveys range from 30 to 80 questions covering all three components across the study topic. Field time estimates for household KAP surveys are typically 35 to 60 minutes. Beyond that, respondent fatigue degrades data quality.
Can KAP data be used to measure behavior change over time?
Yes, when collected at baseline and endline using identical instruments with the same populations or comparable samples. KAP baseline-endline designs are standard in health behavior change program evaluation. The critical requirement is instrument consistency across measurement points.
Newsletter
Personalize your updates! Subscribe to ProjectBist's Newsletter and choose from the following categories.
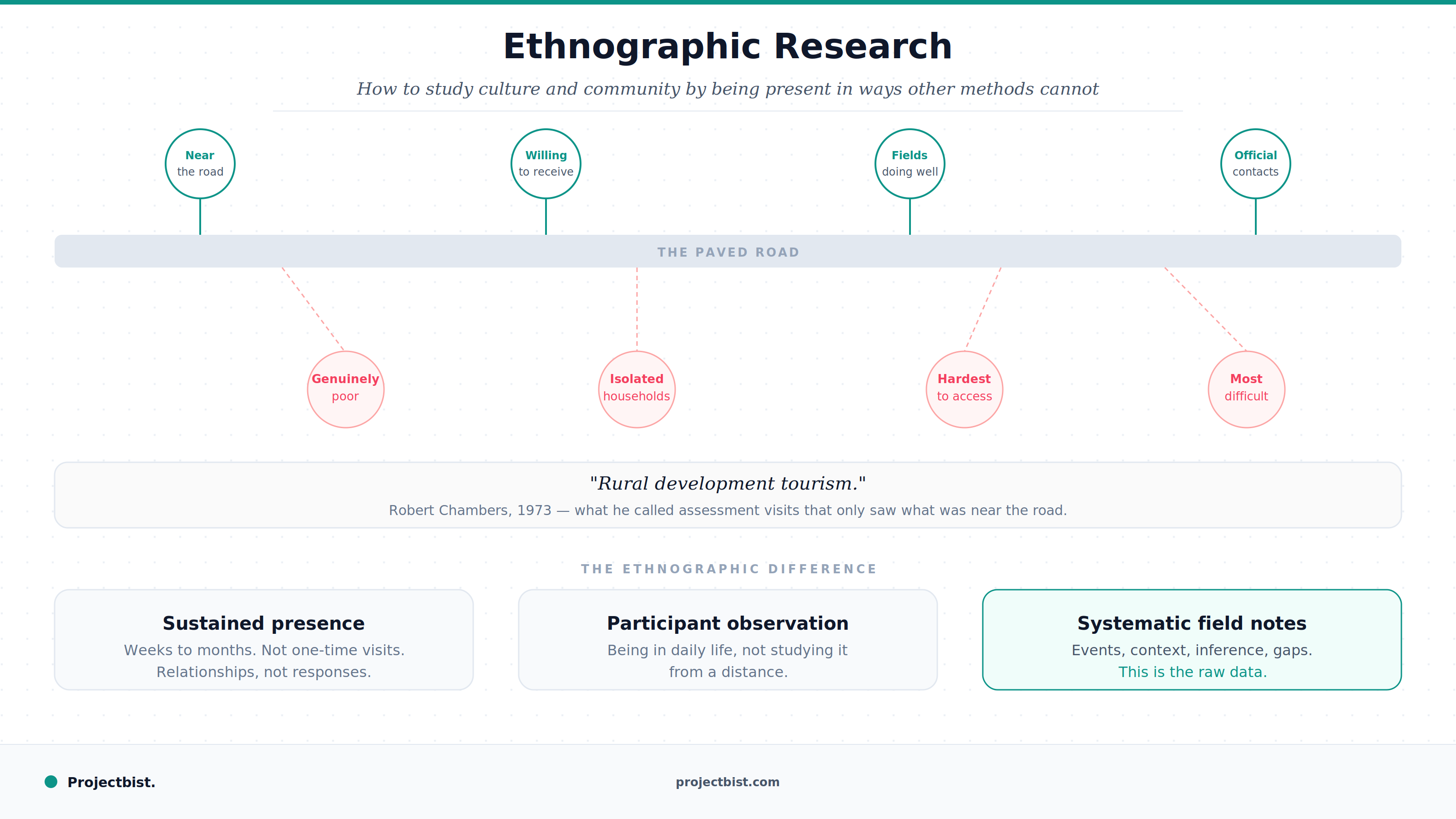
Ethnographic Research: How to Study Culture and Community by Being Present in Ways Other Methods Cannot
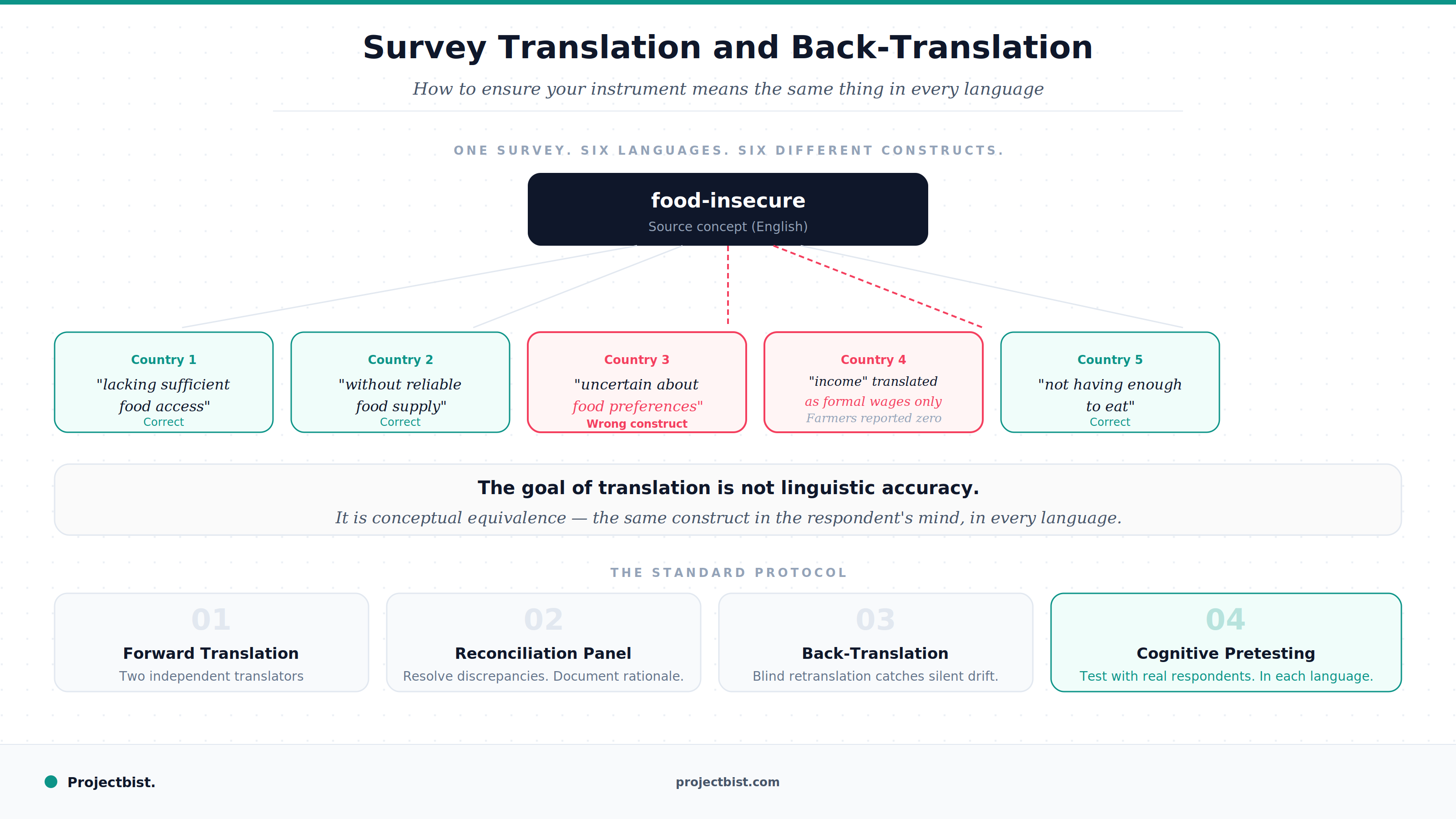
Survey Translation and Back-Translation: How to Ensure Your Instrument Means the Same Thing in Every Language
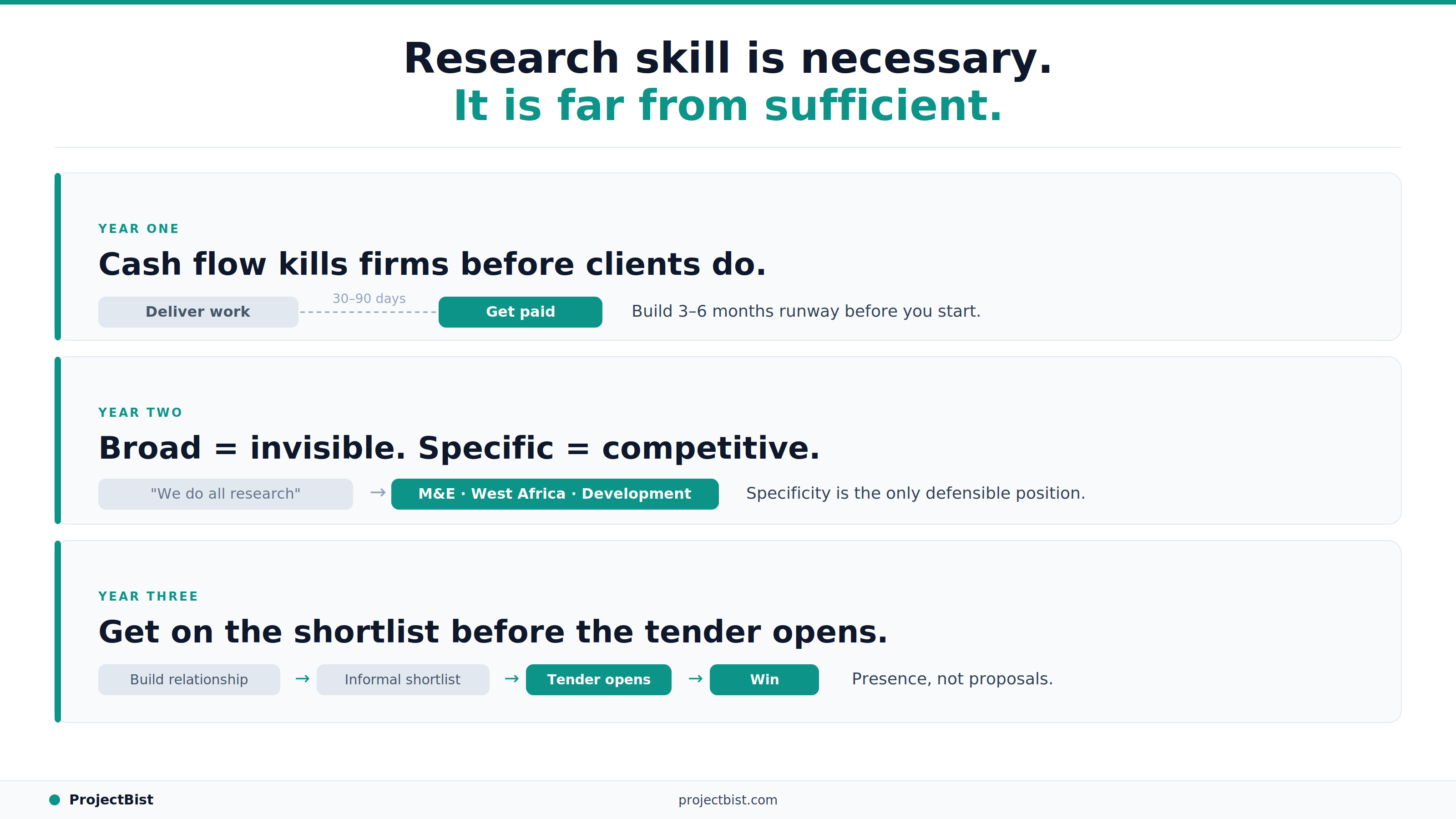
How to Build a Research Firm From Scratch: What the First Three Years Actually Require